Home » Misc » How to prevent acl tear in basketball
How to prevent acl tear in basketball
ACL Tears in Female Athletes: Q&A with a Sports Medicine Expert
Reviewed By:
Women often have unique health care needs, and sports injuries are no exception. Anterior cruciate ligament (ACL) injuries, for example, are more common in women than in men. Johns Hopkins sports medicine expert Andrew Cosgarea, M.D., answers common questions about ACL tears in girls and women and explains what they can do to lower the risk of injury.
How do ACL tears happen?
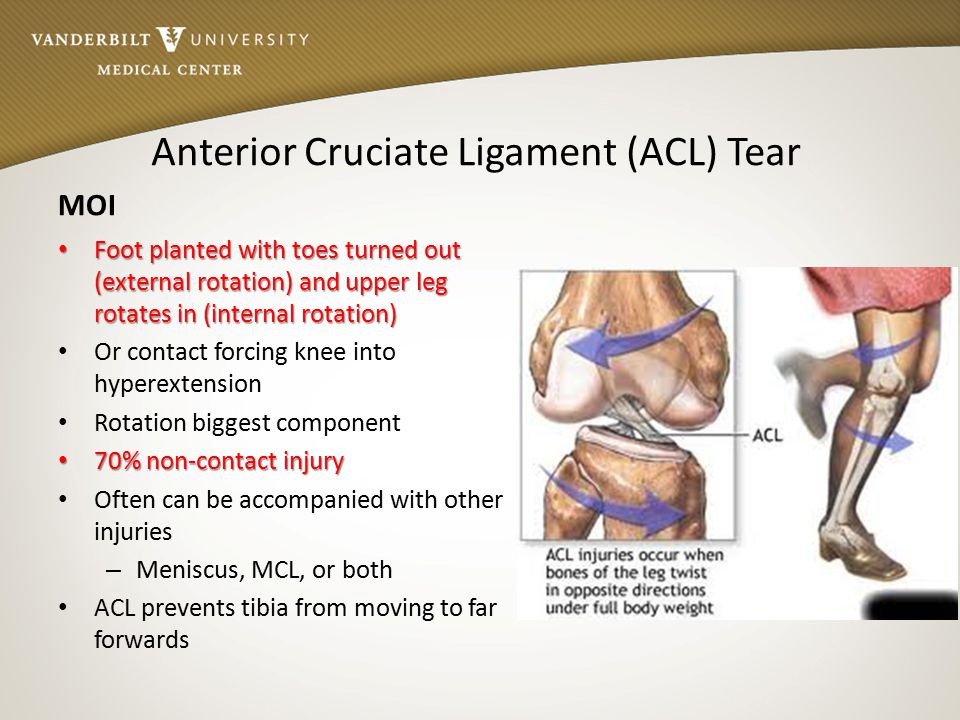
Most of the time, ACL injuries occur in a non-contact fashion, such as quickly changing directions to dodge a defender in soccer or landing from a layup in basketball. The sudden force from a twist or landing may cause the ligament to tear.
Why are ACL tears more common in female athletes?
The structure of the knee joint in women plays a big role in putting them at a higher risk for an ACL tear. Women’s joints — including the knee — generally have more looseness and range of motion than men’s. Women also often have less muscle mass around the knee, contributing to more instability, which can lead to a ligament tear if the ligament gets overstretched.
Technique differences also play a role. When coming down from a jump, female athletes tend to land in a collapsing pattern, moving their knees inward and often not bending them enough. The combination of these factors makes an ACL tear more likely.
Is ACL tear treatment different for female athletes?
The treatment options for ACL tears are the same, regardless of your gender. They typically include physical therapy, anti-inflammatory medications and, often, surgery. However, there is a benefit in working with a sports medicine specialist who understands that the ACL tear mechanism in women is different from how it occurs in men. He or she can provide recommendations to improve technique or strengthen certain muscle groups to help prevent a second injury.
The Johns Hopkins Women’s Sports Medicine Program
The Women’s Sports Medicine Program at Johns Hopkins features experts in nutrition, concussions, orthopaedic surgery, physical therapy and more. Our team understands the unique needs of female athletes and uses a “whole body” approach to treatment.
Learn more about our women’s sports medicine program
Is surgery always necessary after an ACL tear?
Not necessarily. The decision to repair an ACL tear with surgery should factor in age, current activity level and desired activity level. Women who are older and/or don’t participate in many high-intensity sport or leisure activities might get good results from physical therapy alone. Meanwhile, women who play sports or have knee-straining jobs or hobbies, such as dancing, may benefit from surgery to recover as much function as possible and continue their active lifestyle. A sports medicine specialist can help decide which option is best.
Are women more likely to re-tear an ACL?
The same mechanism that led to the first injury can lead to a second one. An ACL tear can happen again, either in the reconstructed knee or in the healthy knee. The quality of the reconstruction, activity level and sport of choice all play a role in reinjury risk.
Unfortunately, it’s still possible to re-tear an ACL that was reconstructed and rehabilitated perfectly. The higher the activity level, the higher the risk.
ACL Surgery | Michelle's Story
What can female athletes do to prevent ACL tears?
Sports injuries are always a possibility, even if you do everything right. But there are steps you can take to minimize risk factors related to your technique, training and lifestyle. The following recommendations are all equally important in preventing ACL tears and other sports injuries:
Practice good technique. While not a guarantee, proper technique when training and playing a sport can help ward off sports injuries. Work with your coach and/or your sports physical therapist to identify improper form and correct it.
Avoid working out while overly fatigued. When you’re tired, it’s easier to make mistakes or forget about good technique. Getting enough sleep and stopping a workout before exhaustion sets in help to prevent injury.
Work to develop muscle groups evenly. Core and extremity strength are equally important. Focusing on one while ignoring the other increases your risk of injury.
Create a balance between strength and flexibility. Both tight and overstretched muscles are more prone to injury. Working on strength and flexibility in moderation is key.
Eat a balanced diet. Poor nutrition leads to decreased strength, endurance and attention. Eating well can help improve your focus and performance.
ACL Prevention Tips - National Basketball Players Association
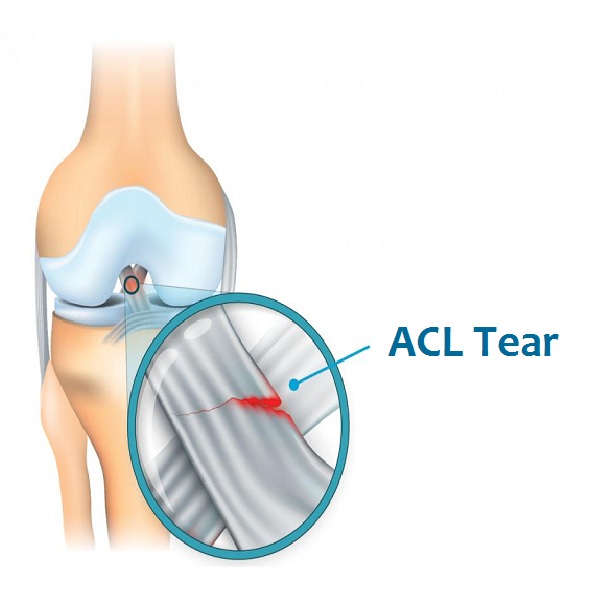
ACL: Three dreaded letters no athlete ever wants to hear.
The ACL, or the Anterior Cruciate Ligament, is an important ligament that functions as a knee stabilizer. When torn in athletes, ACL injuries often lead to surgery, an ended season, and up to a year spent in rehabilitation in order to achieve a successful return to sport. Even then successful return to sport and/or return to prior level of sport function is not guaranteed. A study by Benedict Nwachukwu, MD and colleagues at HSS demonstrated that successful return to sport after ACL reconstruction occurs in 88% of cases.
Given the difficulties associated with ACL rehabilitation and recovery the goal is to avoid these injuries in the first place. Unfortunately, ACL injuries are very common, with between 100,000 to 200,000 occurring each year. In fact ACL tears are non-discriminant and can occur in all ages and sport function types – from the professional athlete to the occasional weekend warrior.
Top players like Klay Thompson, Derrick Rose, Kristaps Porzingis and many other NBA basketball players have sustained ACL injuries in their careers. While there are many promising stories of recovery, the road to get there is not easy!
Everyone is vulnerable, including youth athletes and especially female athletes. In fact, females are two to ten times more likely to suffer an ACL injury than their male counterparts (HSS). The available literature suggests that a number of factors may influence this increased risk in women. Factors include lower extremity alignment, hormonal regulation, intrinsic ACL anatomy and neuromuscular differences.
Luckily, there are ways athletes can help minimize their risk of injury.
Many injury prevention exercises share a common focus: improving strength (especially quads, hamstrings & core), flexibility, balance, proprioception, jumping and landing properly and having good alignment to protect your knees.
To diminish the risk of ACL injury, here are 5 ACL injury Prevention Tips brought to you by HSS & the NBPA Sports Medicine Team.
These exercises should be done routinely, ideally three times per week to help significantly reduce chances of injury.
1. Calf Raises | 30 Reps
Instructions:
Stand upright with your feet hip-width apart and your toes pointing forward.
Raise your heels off the floor and squeeze your calves.
Return to starting position, by slowly lowering your heels, and repeat.
Targeted Muscle: Calves
2. Glute Bridge | 12 Reps
Instructions:
Begin on your back with your knees bent, arms straight beside you, feet flat on the ground.
Engage your core, press your heels to lift your hips until your body is a straight line between your knees and your shoulders. For a more challenging version, lift up with only leg
Hold for two seconds and slowly return to starting position.
Target Muscles: Glutes, Hamstrings, Abdominals
3. Lunges (Forward & Reverse) | 8 Reps each leg
Instructions:
Stand tall with feet hip-width apart. Engage your core. Do two forward lunges followed by two reverse lunges.
Forward Lunge - Take a big step forward with right leg. Lower your body so that your right thigh (front leg) is parallel to the floor and your right knee is positioned directly over your ankle. Your left knee should be bent at a 90-degree angle and pointing toward the floor with your left heel lifted. Return to standing by pressing your right heel into the floor and bring left leg forward. Alternate legs.
Target muscles: Quads and Core
Reverse Lunge - Take a big step backwards with your left foot. Lower your body so that your right thigh (front leg) is parallel to the floor with your right knee is positioned directly over your ankle. Your left knee should be bent at a 90-degree angle and pointing toward the floor with your left heel lifted. Return to standing by pressing your right heel into the floor and bring left leg forward. Alternate legs, step back with right leg.
Target muscles: Glutes and Hamstrings
4. Jump Squat | 10 Reps
Instructions:
Starting with feet hip-width apart, do a regular squat, engage your core, and jump up explosively.
When you land, push your butt back and lower down into a 45 degree squat position to complete one rep.
Once landing properly, repeat the same motion.
Target muscles: Glutes, Hamstrings, Quads, Lower Abs, and Calves
5. Skater Jumps | 6 Each Side
Instructions:
Standing feet shoulder width apart, lift your left knee in the air and get into quarter squat.
Using the momentum from your left leg, jump horizontally to about 2-3 ft, landing on your left leg. Absorb impact for 1-2 secs and repeat the motion with your right leg as lead to complete one rep. Be sure to pump your arms to increase the momentum.
Target muscles: Glutes, Hips, Quads
Injuries aren’t always preventable, but the more time you put into pre-rehabilitation, the less time you will have to work on coming back.
For more information on how to treat and recover from injuries, visit the Hospital for Special Surgery, the #1 Hospital for Orthopedics and Official Hospital of the NBPA.
Dr Benedict Nwachukwu is a contributing author and is a Sports Medicine Surgeon at Hospital for Special Surgery and Medical Consultant for the NBPA. For more information about his surgical practice visit www.manhattansportsdoc.com
Injury to the crosses is a nightmare. In the Premier League, they are torn more and more often, 30% get relapses, and there are a million reasons (even boots) in football.
You should immediately start with the main thing. A torn cruciate ligament is worse than most injuries. As a rule, football players understand everything in the first seconds, even without a medical diagnosis, and often leave the field in tears. Below - dotted line lists the reasons why everyone is so afraid of crosses.
• 70% of such injuries are accidental, crosses are torn suddenly and out of the blue. It's one thing to get injured in a hard joint for the ball (when you go to the fight, you psychologically prepare for everything), and another thing is when you just put your foot unsuccessfully on landing.
• Long and difficult rehabilitation. To recover from such an injury, you need at least six months, and the first months of almost every exercise are accompanied by severe pain and require great effort.
• You may not play at the same level after an injury. It's one thing to recover and quite another to get back in better shape. Such situations harden someone, and break someone.
• Frequent relapses. Nearly a third of all players who tore crosses experienced re-injury to crosses or tore them on the other leg.
Sports doctor Zurab Ordzhonikidze combined all these theses into one succinct sentence: "A cross injury for a football player is like a myocardial infarction for an ordinary person."
New stories appear almost every week, one of the most recent examples is Depay, who had a delightful autumn part of the season, but by the end of the year broke his crosses and will now miss the Euro. And the match of the 19th round of Serie A "Roma" - "Juventus" is generally a real drama. With a difference of 19 minutes, two young football players of both clubs flew out with crosses - Roman midfielder Nicolo Zaniolo (20 years old) and Turin defender Merih Demiral (21 years old). Now they have an operation and six months of rehabilitation ahead of them instead of fighting for a place at the base.
Cross injuries are even more common than you think and cost clubs a lot of money
Anterior cruciate ligament tears account for 20. 5% of knee injuries and 3% of all injuries in football.
In 2017, the BBC conducted a study and found that the number of knee ligament injuries in the Premier League is increasing every year.
In each of the studied years, knee ligament injuries were among the three most common injuries, second only to musculotendinous ones. In the same 2017, the website SportingIntelligence.com and the insurance company JLT found out that cruciate ligament injuries are not only a blow to the athlete's career, but also to the club's budget. In the 2016/17 season alone, the Premier League spent £177m on the salaries of players undergoing rehabilitation.
“Over the past six seasons, the cost of cruciate ligament injuries has steadily increased as players become more expensive. It annoys the clubs, but they can't change the situation," explained JLT sports director Duncan Fraser.
It turns out that an injury to the cruciate ligaments is a problem not only for a player, but also for his club, and for sports in general. Players cost more and more and get injured more often. Is there nothing that can be done about it? To do this, you need to understand the root of the problem.
What are these ligaments responsible for? Why is their breakup so painful?
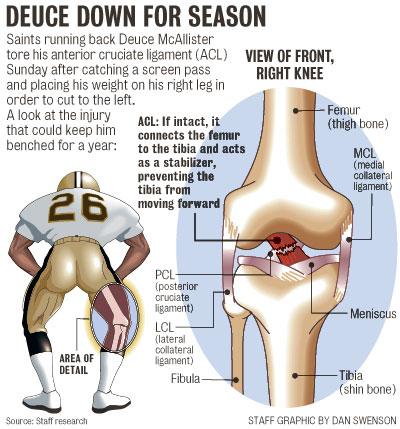
Figure shows right knee, front view, joint capsule and patella removed for convenience.
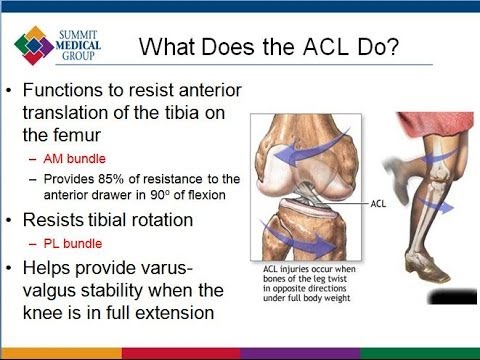
Pathology cannot be disassembled without knowledge of the norm. Therefore, a small anatomy course - the anterior cruciate ligament starts from the inner surface of the external condyle (bone protrusion) of the femur, crosses the knee joint and attaches to the anterior part of the anterior intercondylar fossa of the tibia. And now in Russian: this ligament stabilizes the knee joint and prevents the lower leg from moving forward excessively.
The posterior one starts from the lateral surface of the inner condyle of the thigh, crosses the knee joint and attaches to the posterior intercondylar fossa of the tibia. And again in Russian: it stabilizes the knee joint, and keeps the lower leg from moving backward. An important detail is that the posterior ligament is much thicker, which is why its injuries are much rarer in sports (for 1 injury to the posterior ligament, there are about 20 ruptures of the anterior ligament).
Collateral ligaments (outer and inner) keep the lower leg from moving in and out, respectively. Often their rupture is combined with an injury to the cruciate ligaments.
In addition, the thigh muscles also stabilize the knee. The main role here is played by the four-headed.
It has 4 heads (so powerful it's more like 4 separate muscles with a common point of attachment) and they can generate enough traction to stabilize the knee even with a torn or missing ACL, but more on that later.
How does cruciate ligament rupture occur?
The mechanisms of their damage can be divided into 2 groups:
1. Contact: impacts, collisions and so on. In the case of a contact injury, everything is quite simple - it is a direct blow to the lower leg or a fall on it. At this moment, the body moves in one direction, the lower leg in the other. If the force is strong enough, then the ligament does not withstand and breaks.
There is a rupture of the ligament in which direction the movement of the lower leg occurs - the anterior forward, the posterior - backward. This is how about 30% of these injuries occur.
2. Non-contact: falling, sudden change of direction, braking, landings. This is about 70% of cruciate ligament injuries. With a fixed shin, the femur rotates inward, or the shin and foot tuck and rotate outward.
It is much easier to show it on video:
In both cases it is accompanied by:
• click, crunch or something similar;
• severe pain at the time of injury and when walking;
• a feeling of instability in the knee: when you try to lean on the injured leg, it tucks.
What scares me the most is how serious an injury you can get out of the blue. In addition, since everything in our body is interconnected (especially the joints), the force that can tear a ligament rarely falls strictly on one cruciate and therefore an isolated injury to only one ligament is a rare occurrence. Much more often, along with the crosses, the menisci and lateral ligaments are torn, as was the case, for example, with Djordjevic - this is called the “unlucky” Turner triad (Soviet surgeon and orthopedist).
It is called unlucky for two reasons: firstly, due to the proximity of the medial meniscus, the medial lateral ligament (they are even fused to each other) and the anterior cruciate ligament, their simultaneous rupture is quite common when the anterior cross is torn. And secondly, such an injury requires a longer recovery, since there is a pronounced instability of the knee joint, practically nothing keeps it from pathological movements inward and forward.
Ibra is a perfect example of non-contact breaking of crosses. Because of him, Zlatan left Europe and lost his former greatness. Three years ago, 34-year-old Zlatan just hit the ground running, and in his first English season he scored 28 goals in 46 matches. Manchester United were preparing to extend his contract. But one evening spoiled everything - April 20, 2017. United took on Anderlecht in the UEFA Champions League quarter-finals. Closer to the final whistle, Zlatan fought for a high ball in the penalty area, landed badly and went to the hospital with a torn right knee cross.
The most likely option at this age is to finish playing football. But Ibra was determined to return and even went for a consultation with the famous sports doctor and professor at the University of Pittsburgh - Freddie Fu. He was delighted with Zlatan's body and convinced the Swede that he would return to football: “The morphology of his health, his bones and muscles are all as perfect as you can imagine. He is one of the best athletes I have ever worked with, he is in great shape. "
Ibra took up training with great enthusiasm - he often came to Manchester United's base even at night. Zlatan returned after 9 months, and in absolutely his own style: in the first match he hit with scissors, and after the game he called himself a lion.
It seems that Zlatan remained a beast, but this is not entirely true: he played only one match at the start of Manchester United, scored one goal and promptly left for MLS, a league with a much lower pace.
“ Zlatan came back different,” Mourinho said after leaving Manchester United. – He lacked speed and sharpness, he lost to our young players . I saw in him doubts and self-doubt, he understood that he was no longer so strong.
Are crosses always torn by accident? Are there any prerequisites?
At risk are football players, American football players, skiers and in general any contact sport. You may ask, what does contact sports have to do with skiing? What is the contact? But have you ever seen skiers fall? The leg goes in one direction, and the body rotates by inertia in the other. Yes, yes, again the same mechanism, because the boot, like a boot, fixes the lower leg.
This is why this injury is sometimes referred to as "ski boot injury".
More one interesting fact: in women, the risk of cruciate ligament injury is about three times higher than (just yesterday Ada Hegerberg tore her crosses). This issue has not been fully studied, there are many different theories related to anatomical features, hormonal regulation, the ability to coordinate, but in general it all comes down to a simple one: “a man is stronger, he has more testosterone (the male sex hormone is also responsible for strength). muscles and ligaments), which means stronger ligaments and muscles.
The suddenness of this injury is frightening, but several risk factors can still be identified - when the likelihood of breaking the crosses increases.
• When the thigh muscles are not strong enough. Strong muscles can in many cases save you from injury, but still do not guarantee this.
• When the thigh muscles are damaged. Tired, weak muscles, untreated injuries - all this increases the risk of damage to the ligaments.
• When coordination is not at the top level. The ability to control your body (especially when jumping) can help avoid one of the mechanisms of injury, but again: in football, you usually do not allow free jumping and landing in the fight for a high ball. It really needs mastery of the body.
• When playing on artificial turf. Wet synthetic fields turn into a real ice rink. It's easy to get lost here.
• When the spikes are not picked up well. The role of spikes in football is obvious - it is a stable good grip on the lawn. If you use too short ones - the leg can go, turn up - a vivid example of a non-contact mechanism. But too much grip can also interfere - not only will such shoes slow down, but also increase the risk of tripping due to the fact that the foot literally hit the ground. The RFU even has special recommendations for the selection of shoes.
There is a high chance of re-injury if the crosses are torn. Giuseppe Rossi was a Serie A star and almost moved to Barça, but two relapses killed his career
A few years ago, the Stockholm Sports Injury Research Center, with the support of the Westmanland Regional Hospital, studied the impact of a cruciate ligament injury on the later career of football players.
The numbers are so-so: among those who returned to football, almost a third (30.3%) again faced an injury to the crosses. 9.7% - received repeated damage to the anterior cruciate ligament, 20.6% - torn the anterior cruciate ligament on a healthy leg. A striking example is Giuseppe Rossi.
In the mid-2000s, the Italian striker was considered a United supertalent: Ferguson called him a future Old Trafford legend, Ronaldo admitted that he was a little jealous.
But it didn't work out at Manchester United - after a couple of loan spells, Rossi moved to Villarreal, where he finally began to open up: in the amazing 2010/11 season, he scored 18 goals. Rossi was only 23 at the time, and the Premier League was back on the horizon with Manchester United retaining the right to buy Giuseppe for £10m and Liverpool looking for a striker.
But everything changed in October 2011. Then Rossi left the field in a match with Real Madrid because of strange sensations in his knee. As a result, Villarreal flew 3-0, and an MRI showed Rossi had a cruciate ligament rupture.
Six months later, the striker was ready to return, but there was a relapse during training. And that meant at least another 10 months without football. As a result, Giuseppe missed 557 days, during which he managed to fly past Euro 2012 and change from Villarreal to Fiorentina. Rossi finally returned only at the start of the 2013/14 season: amazingly, even after a year and a half without football, he remained a goal-scoring striker.
By January 2014, Giuseppe had already become a superstar in Serie A - 16 goals in 17 matches (among them a hat-trick against Juventus), Vincenzo Montella's admiration (the Fiorentina coach called Rossi a "true genius") and interest " Bayern and Barca. The fairy tale ended in the January match against Livorno: defender Ricardo Rinaudo went into a hard joint and Rossi tore the crosses again. On the same knee.
This time the miracle didn't happen – after a year and a half Giuseppe came back slow, traveled around the middle peasants in Spain and Italy, almost didn't score and really didn't come out at the start.
The impact of the second broken crosses on Rossi's game is perfectly illustrated by the statistics:
In April 2017, in a match against Eibar, Rossi landed badly and broke the crosses for the third time - in fact, this injury ended his career. Now Giuseppe is 33, he does not have a contract, and only the title of the best scorer in the history of Villarreal reminds of his fighting youth.
“Honestly, it is very difficult for me to remember the nightmare that I experienced over and over again. Every injury has a sad story - either I missed the World Cup and the Euro, then the transfer to the top club failed . .. These fucking injuries always interfered.
Rossi has collected a complete collection of failures: two recurrences of crosses and a set of other serious injuries. Giuseppe Rossi is a perfect example of how an ACL tear turns ambition and talent into a void.
Is breaking a cross almost always the end of a career?
Of course not. How an athlete handles a cruciate ligament injury depends on many factors, most notably the athlete and their relationship to injury and rehabilitation.
There are several football players in history who got this injury and quickly forgot about it.
• Alessandro Del Piero injured his knee ligaments at 24, but returned and even said that the injury made him stronger:
“I used to play mostly instinctively, but after the injury I learned to control my instincts. There is more balance in my game."
• Lahm tore his crosses shortly after returning to Bayern, but soon forgot about the injury and made over 300 appearances for the Munich side, helping them win the Champions League. It also happened in the national team - in 2014 Lam became the world champion with Germany.
• Although Ronaldo's career was ruined by injury, the Brazilian is still regarded as one of the greatest strikers in history, having enjoyed several top seasons since injury (including World Cup gold medals).
• Alan Shearer broke his crosses before his second season at Newcastle but returned to become a club legend with over 300 appearances and 148 goals.
• Ruud van Nistelrooy may never have moved to Manchester United - PSV and Mancun had barely agreed on a transfer when it turned out that the striker had a serious knee injury. The British did not refuse the player and waited for him for almost a year. Not for nothing: the striker broke the record of Shearer and Henry, scoring in 8 league matches in a row, and then improved this result by extending the streak to 10 goalscoring games. Van Nistelrooy won absolutely every English trophy with Manchester United.
Is tearing up crosses always an operation? Is it possible to get by?
It is possible, but in professional sports it is not relevant: to achieve good knee stability, muscle strength in such a situation is not enough.
What happens during the operation? Surgeons remove the stump of the torn ligament so that it does not interfere with movement, take a graft from the patellar ligament (it is long enough and at the same time wide enough to easily cut off part of it), drill holes in the femur and tibia, where the graft is placed, which exactly repeats the course of the "native" ligament.
It all looks like this:
You can do without surgery only if there is a tear and if the knee remains stable at the same time. In this case, the athlete pumps the quadriceps muscle, which compensates for this partial tear, further stabilizing the knee.
But in the case of professional athletes, if he flatly refuses to operate, the doctor simply waits for the patient to return with a completely torn ligament. In professional sports, leaving an athlete with a torn ligament is practically a guarantee of a complete rupture in the future.
Rehabilitation after breaking the crosses is sheer pain, you need maximum dedication and great willpower
And then the most difficult stage. He was well described by Roman Zobnin when he injured his ligaments in 2017.
“The most difficult time is the first week after the operation,” the footballer recalled. - I could not sleep and walk normally, I did everything through pain. It was painful. Even the enemy will not wish what I suffered. But with every day of training it becomes significantly better. ”
Since the rehabilitation process is quite complex, it is divided into stages.
• The first weeks after the operation, starting literally on the second day, the main task is to restore the full range of motion, eliminate pain and relieve swelling, mainly these are minimal loads, massage, passive movements (i.e., performed without effort, they are performed by a massage therapist or doctor). This is the most important and difficult stage, since absolutely any exercise associated with the slightest effort provokes severe pain.
• By the end of the first month, the range of motion should be restored and work on strengthening the thigh muscles, coordination begins, gradually adding a bicycle, an elliptical trainer, if possible, exercises in the pool and aquabike. For example, this is what Depay can already do after just a month.
View this post on Instagram
1 month ✅
A post shared by Memphis Depay (@memphisdepay) on Jan 19, 2020 at 12:00pm PST
Then it's a little easier - the main task of the remaining period of rehabilitation is the restoration of muscle strength, the introduction of more and more complex exercises and a full return to normal training. From 2 months, you can add exercises on the treadmill (low speeds, mostly a step, without a slope), from 3-4 months, running, agility exercises begin, and after 4-5 months, the athlete is already able to endure running loads without pain. By 5-6 months, the footballer is generally able to return to the loads of the general group.
Cruciate ligaments can also be torn during a yard match. Here are ways to protect yourself
It is important to remember that knee ligament injuries are not only a problem for professional football players, but also for ordinary people who went out to play on the next box.
100% protection against such damage will not work, but there are a number of rules that will reduce the chances of getting to know the arthroscope and are quite applicable for amateurs. Keep a few things in mind.
• Warm-up is required. This is a general rule for the prevention of any injury.
• Strong thigh muscles help take pressure off the knee. First of all, this concerns the quadriceps muscle, which, as mentioned above, additionally stabilizes the knee. So matches on the box should be combined with trips to the gym or independent exercises to strengthen leg muscles.
• Proprioception training. And now in Russian. Proprioception is the feeling of the position of your own body parts relative to each other and in space, in other words, the ability to understand what your hand is doing, even if it is behind your back. And what about injuries? It's very simple - a developed proprioceptive sense helps to better control your body and, in general, is indispensable for a top-level football player. Here is a good set of exercises.
• Keep an eye on machinery. This applies to anything, running technique, jumping, exercises in the gym. The technique of performing exercises should be perfected to automatism, quality should be more important than quantity - it is better to do less, but correctly.
• Get adequate rest and sleep. A tired muscle is naturally weaker than a normal one. A tired person tends to make mistakes: stumble, get distracted, think.
Photo: East NewsClaudio Pasquazi/Anadolu Agency/ABACAPRESS.COM; RIA Novosti/Alexander Wilf; Gettyimages.ru/Laurence Griffiths, Valerio Pennicino, Martin Rose/Bongarts
ACL injuries: methods of treatment and recovery
Anterior cruciate ligament (ACL) is located in the central part of the knee joint, perpendicular to the back. Together they form a cruciform structure. Being one of the main stabilizers, the ACL helps to keep the lower leg from moving forward and inward, thereby ensuring the stability of the knee joint. Ligament injuries are often diagnosed in basketball players, hockey players, figure skaters, football players, skiers, and those involved in contact sports. It usually occurs when the supporting leg rotates excessively at the knee joint due to an unsuccessful movement or a strong side impact.
This injury is widespread, and in terms of the number of recorded cases, it exceeds damage to the menisci (Achilles tendons) - out of 100,000 patients, 30 turn to specialists with ACL rupture. Often there are combined cases, when other parts of the joint are damaged along with the ligaments.
Basic Treatments
ACL rupture is treated conservatively and surgically. Depending on the severity of the injury, the doctor may prescribe the patient only conservative treatment or emergency surgery. A combination of these two methods also takes place.
Conservative treatment depends on the duration of the injury and is divided into stages:
The first - a few days after the injury - swelling and pain are relieved by taking anti-inflammatory and analgesic drugs. When a pronounced hermatosis is detected (blood enters the cavity of the knee joint), the accumulated fluid must be removed. In the first days after the injury, any load on the sore leg is strictly prohibited in order to avoid even more injury. At this time, doctors recommend wearing a plaster splint that fixes the knee.
The second - 3-5 weeks - is aimed at restoring the motor function of the joint. In order to prevent muscle atrophy (exhaustion) and restore stability to the knee, the rehabilitation doctor prescribes a course of physiotherapy and therapeutic exercises. But if other elements of the joint were damaged with the rupture of the ACL, then you have to resort to surgery.
Conservative treatment is considered successful when the joint is fully restored upon its completion.
Surgical treatment
If therapy fails to achieve a stable state, then surgical intervention is prescribed. In such a situation, a high-tech, minimally invasive operation is prescribed - arthroscopy. When it is performed, a new cruciate ligament is created from its own tissues (tendons) through small punctures in the joint. The process of manipulations is controlled through a mini-video camera (arthroscope). This approach makes it possible to preserve the integrity of nearby structures, while simultaneously diagnosing and creating a new bundle.
Immediate surgery without medical therapy is indicated for athletes or if the patient has severe damage to other tissues with ACL rupture, which prevents a full-fledged conservative treatment.
Anterior Cruciate Ligament Injury Rehabilitation
State of the art equipment for ligament surgeries can achieve great results. However, it is important to understand that the treatment of ACL injuries is impossible without rehabilitation. The long-term functional stability of the knee depends on the nature of the rehabilitation. Rehabilitation after ACL rupture in the Artromed clinic in Odessa is carried out according to an individually developed program compiled by an experienced rehabilitation specialist. The selection of restorative techniques and exercises is carried out taking into account the nature of the injury, the presence of other injuries and the method of treatment.
Rehabilitation after conservative treatment
If the treatment of PKC was carried out by a conservative method, then the rehabilitation will last 6-8 weeks. The program is aimed at:
Reduced pain and swelling.
Restoration of full range of motion of the knee.
Muscle strengthening.
Correction of knee instability.
The achievement of the result is facilitated by the appointment of the following procedures to the patient by the doctors of the Artromed clinic:
application of compresses;
physiotherapy activities;
physiotherapy exercises (LFK).
You will perform all procedures under the supervision of a rehabilitation doctor at the Artromed clinic.
Rehabilitation after surgical treatment
Rehabilitation after surgical treatment is quite long - about 6 months. The main part of rehabilitation is aimed at performing special physical exercises, therefore, for athletes who initially had a high level of physical fitness, recovery can be faster, and for patients who are not involved in sports, it can be longer.
The standard rehabilitation course is divided into 5 stages, the purpose of which is:
In the first stage: reduce pain and swelling in the joint; improve passive range of motion in the joint; regain control of the thigh muscles; improve proprioception of the joint; achieve the ability to walk without crutches; eliminate the difficulty of "turning on" the inner part of the quadriceps femoris muscle; improve peripheral circulation and increase the contractility of the quadriceps femoris.
In the second step: completely eliminate swelling; return full range of motion; improve thigh muscle strength; improve proprioception and joint balance; achieve complete control when walking.
In the third step: improve muscle strength, power and endurance without pain; gradually return functional activity in the sport in which the patient is engaged, if he is an athlete; resume normal running ability.
In the fourth step: restoration of the full range of active movements; elimination of pain and swelling during physical activity; return of maximum strength and endurance, neuromuscular coordination.
The fifth stage is the most important for professional athletes, since it is important for them not only to restore the functions of the knee joint, but also to continue their sports activities, return to full-fledged training and not be afraid of further complications. Therefore, at the fifth stage, the rehabilitologist draws up a special program for the restoration of fitness. The program is aimed at acquiring a high general preparedness, restoring the technical and tactical skills of an athlete.
Rehabilitation of the patient after knee surgery is accompanied by such procedures as:
Magnetotherapy
Electromyostimulation
Foot massage
Active mechanotherapy
Artromed Medical Center in Odessa cares about your health, so the rehabilitation of ACL injuries is carried out by:
qualified personnel;
according to an individually selected program, under the supervision of a doctor;
on the latest equipment;
according to modern European methods;
during the entire rehabilitation period, the patient is under the constant supervision of doctors, which allows you to quickly restore the functions of the knee joint.
Your doctor-rehabilitologist at the Artromed clinic and the traumatologist who performed the operation are always in touch.


 Our team understands the unique needs of female athletes and uses a “whole body” approach to treatment.
Our team understands the unique needs of female athletes and uses a “whole body” approach to treatment. The quality of the reconstruction, activity level and sport of choice all play a role in reinjury risk.
The quality of the reconstruction, activity level and sport of choice all play a role in reinjury risk.  Work with your coach and/or your sports physical therapist to identify improper form and correct it.
Work with your coach and/or your sports physical therapist to identify improper form and correct it.

 For a more challenging version, lift up with only leg
For a more challenging version, lift up with only leg Lower your body so that your right thigh (front leg) is parallel to the floor with your right knee is positioned directly over your ankle. Your left knee should be bent at a 90-degree angle and pointing toward the floor with your left heel lifted. Return to standing by pressing your right heel into the floor and bring left leg forward. Alternate legs, step back with right leg.
Lower your body so that your right thigh (front leg) is parallel to the floor with your right knee is positioned directly over your ankle. Your left knee should be bent at a 90-degree angle and pointing toward the floor with your left heel lifted. Return to standing by pressing your right heel into the floor and bring left leg forward. Alternate legs, step back with right leg. 


 5% of knee injuries and 3% of all injuries in football.
5% of knee injuries and 3% of all injuries in football.  Players cost more and more and get injured more often. Is there nothing that can be done about it? To do this, you need to understand the root of the problem.
Players cost more and more and get injured more often. Is there nothing that can be done about it? To do this, you need to understand the root of the problem. 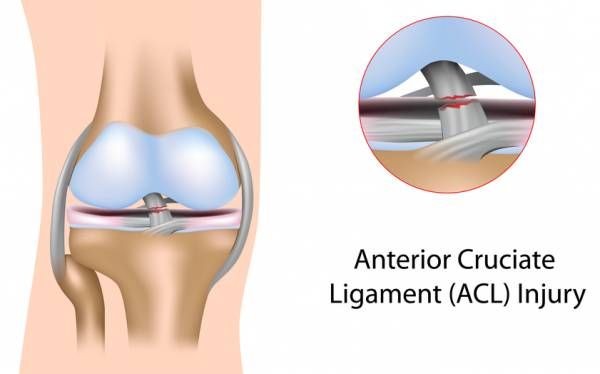 An important detail is that the posterior ligament is much thicker, which is why its injuries are much rarer in sports (for 1 injury to the posterior ligament, there are about 20 ruptures of the anterior ligament).
An important detail is that the posterior ligament is much thicker, which is why its injuries are much rarer in sports (for 1 injury to the posterior ligament, there are about 20 ruptures of the anterior ligament).  At this moment, the body moves in one direction, the lower leg in the other. If the force is strong enough, then the ligament does not withstand and breaks.
At this moment, the body moves in one direction, the lower leg in the other. If the force is strong enough, then the ligament does not withstand and breaks. 
 Because of him, Zlatan left Europe and lost his former greatness. Three years ago, 34-year-old Zlatan just hit the ground running, and in his first English season he scored 28 goals in 46 matches. Manchester United were preparing to extend his contract. But one evening spoiled everything - April 20, 2017. United took on Anderlecht in the UEFA Champions League quarter-finals. Closer to the final whistle, Zlatan fought for a high ball in the penalty area, landed badly and went to the hospital with a torn right knee cross.
Because of him, Zlatan left Europe and lost his former greatness. Three years ago, 34-year-old Zlatan just hit the ground running, and in his first English season he scored 28 goals in 46 matches. Manchester United were preparing to extend his contract. But one evening spoiled everything - April 20, 2017. United took on Anderlecht in the UEFA Champions League quarter-finals. Closer to the final whistle, Zlatan fought for a high ball in the penalty area, landed badly and went to the hospital with a torn right knee cross. 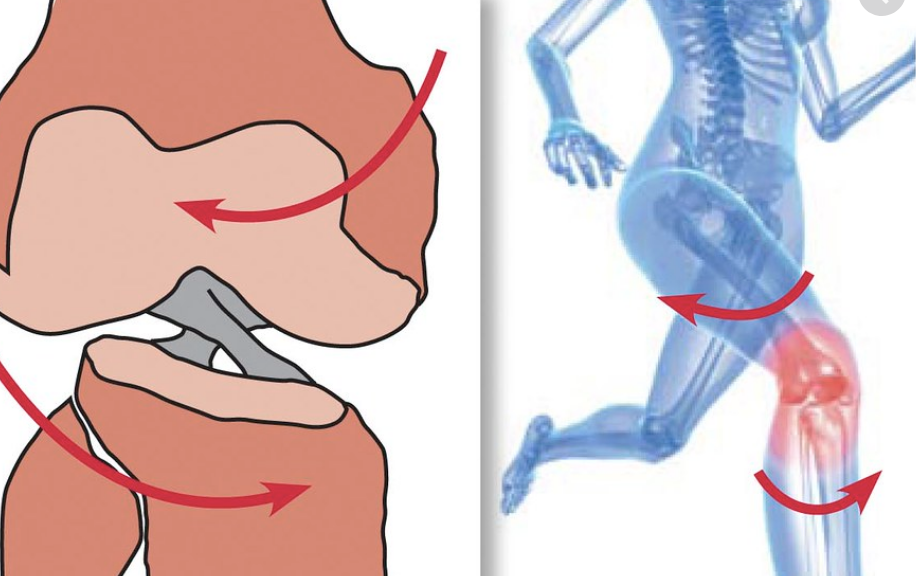 "
"  Yes, yes, again the same mechanism, because the boot, like a boot, fixes the lower leg.
Yes, yes, again the same mechanism, because the boot, like a boot, fixes the lower leg. 
 Rossi was only 23 at the time, and the Premier League was back on the horizon with Manchester United retaining the right to buy Giuseppe for £10m and Liverpool looking for a striker.
Rossi was only 23 at the time, and the Premier League was back on the horizon with Manchester United retaining the right to buy Giuseppe for £10m and Liverpool looking for a striker.  The fairy tale ended in the January match against Livorno: defender Ricardo Rinaudo went into a hard joint and Rossi tore the crosses again. On the same knee.
The fairy tale ended in the January match against Livorno: defender Ricardo Rinaudo went into a hard joint and Rossi tore the crosses again. On the same knee.  .. These fucking injuries always interfered.
.. These fucking injuries always interfered. 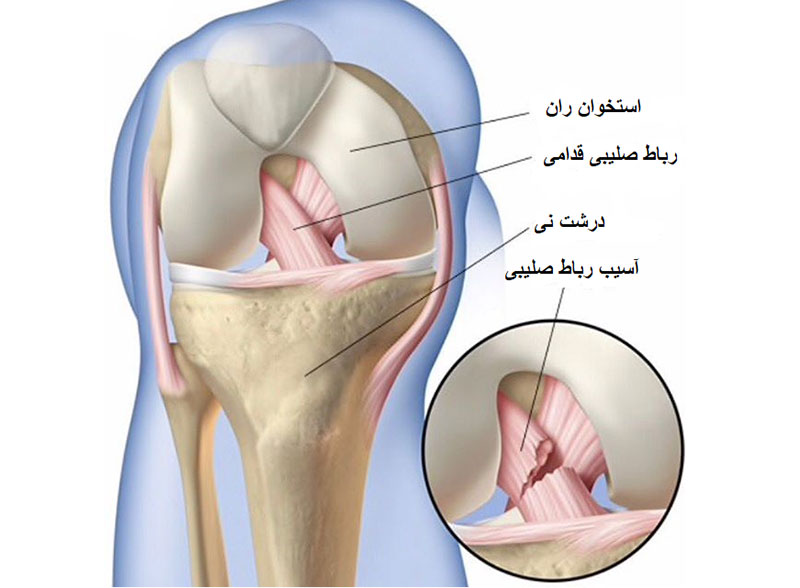 It also happened in the national team - in 2014 Lam became the world champion with Germany.
It also happened in the national team - in 2014 Lam became the world champion with Germany. 


 And what about injuries? It's very simple - a developed proprioceptive sense helps to better control your body and, in general, is indispensable for a top-level football player. Here is a good set of exercises.
And what about injuries? It's very simple - a developed proprioceptive sense helps to better control your body and, in general, is indispensable for a top-level football player. Here is a good set of exercises.  Together they form a cruciform structure. Being one of the main stabilizers, the ACL helps to keep the lower leg from moving forward and inward, thereby ensuring the stability of the knee joint. Ligament injuries are often diagnosed in basketball players, hockey players, figure skaters, football players, skiers, and those involved in contact sports. It usually occurs when the supporting leg rotates excessively at the knee joint due to an unsuccessful movement or a strong side impact.
Together they form a cruciform structure. Being one of the main stabilizers, the ACL helps to keep the lower leg from moving forward and inward, thereby ensuring the stability of the knee joint. Ligament injuries are often diagnosed in basketball players, hockey players, figure skaters, football players, skiers, and those involved in contact sports. It usually occurs when the supporting leg rotates excessively at the knee joint due to an unsuccessful movement or a strong side impact.  A combination of these two methods also takes place.
A combination of these two methods also takes place. 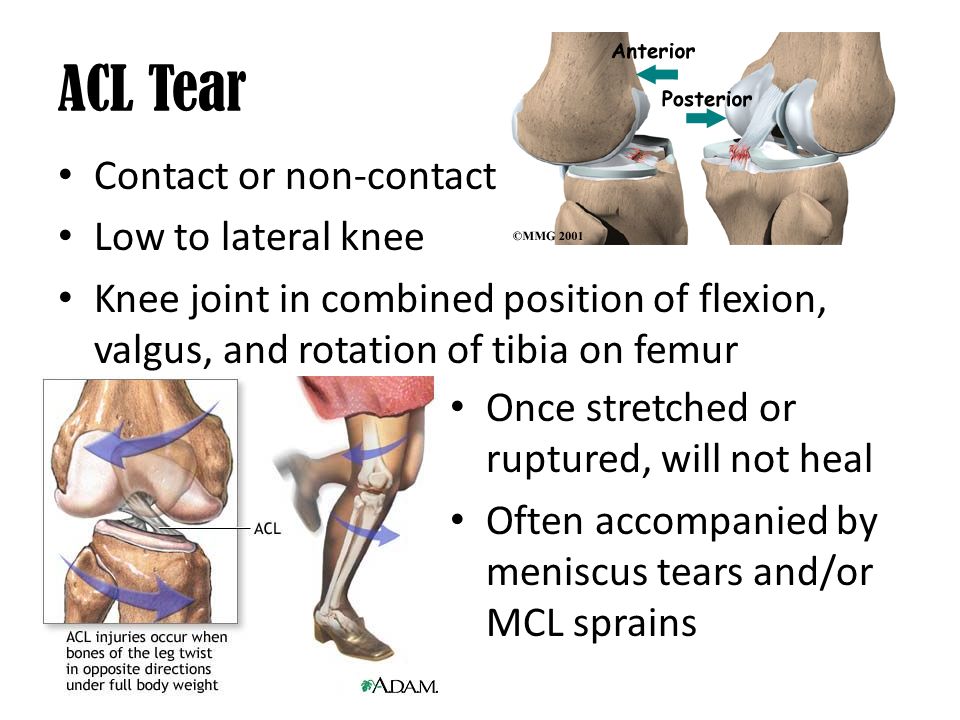
 The long-term functional stability of the knee depends on the nature of the rehabilitation. Rehabilitation after ACL rupture in the Artromed clinic in Odessa is carried out according to an individually developed program compiled by an experienced rehabilitation specialist. The selection of restorative techniques and exercises is carried out taking into account the nature of the injury, the presence of other injuries and the method of treatment.
The long-term functional stability of the knee depends on the nature of the rehabilitation. Rehabilitation after ACL rupture in the Artromed clinic in Odessa is carried out according to an individually developed program compiled by an experienced rehabilitation specialist. The selection of restorative techniques and exercises is carried out taking into account the nature of the injury, the presence of other injuries and the method of treatment. 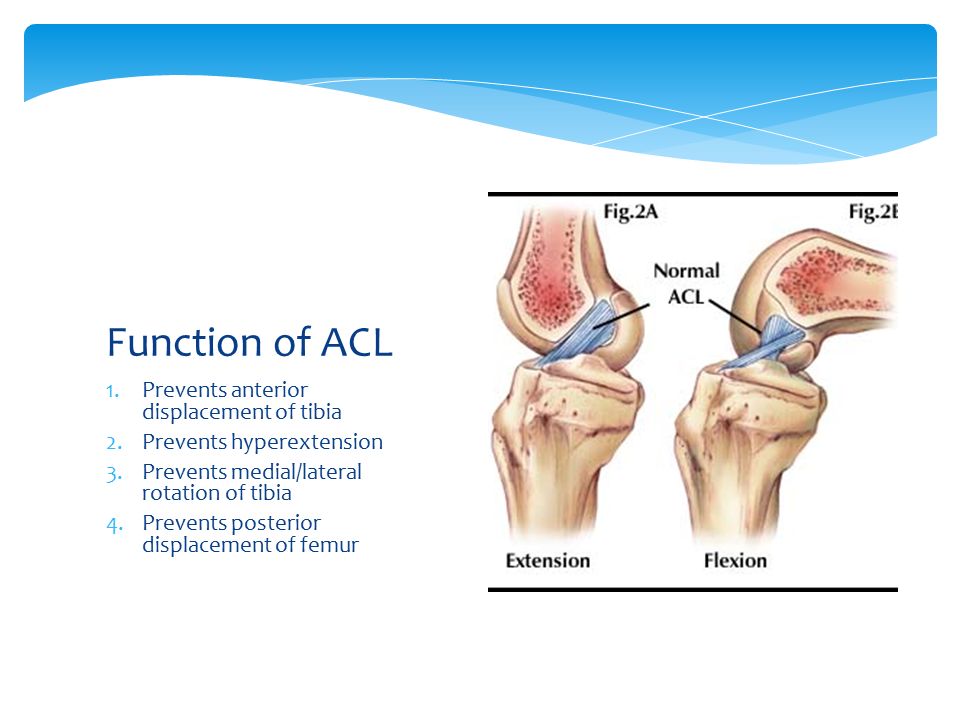
 The program is aimed at acquiring a high general preparedness, restoring the technical and tactical skills of an athlete.
The program is aimed at acquiring a high general preparedness, restoring the technical and tactical skills of an athlete.